Staghorn calculi are complex renal stones that occupy the majority of the renal collecting system. These stones are associated with high morbidity and can lead to recurrent urinary tract infections, urosepsis, renal deterioration, and death if left untreated. Managing patients with staghorn calculi can be challenging. Fortunately, advances in technology and endourology techniques like PCNL have enabled urologists to effectively treat these stones with minimal morbidity to the patient. If you are looking for the best urology hospital in Hyderabad for PCNL Treatment, plus LASER Lithotripsy, Dr Vamsi Urology clinic is the place to be.
Treatment for Staghorn Calculi by PCNL
Treatment is often complicated for Staghorn calculi, but necessary given that untreated stones can lead to recurrent urinary tract infections, urosepsis, renal deterioration, and death. Staghorn calculi were historically thought to be primarily struvite, but modern investigations reveal they can be one of many compositions. These stones are still often associated with infection and urea-splitting organisms. The treatment goal for most patients is complete stone removal to prevent regrowth on persistent stone debris. However, achieving a stone-free state can be difficult, requiring a staged or combined approach.
Imaging
Imaging is a critical step in the evaluation of patients with staghorn calculi. Computed tomography (CT) scan without intravenous contrast is the imaging modality of choice when evaluating a patient for renal calculi that may need intervention. Preoperative imaging is imperative for surgical planning and can aid in choosing what intervention is most appropriate. CT imaging allows for accurate assessment of stone morphology and location, which helps guide percutaneous access when percutaneous nephrolithotomy (PCNL) is planned.
Characteristics of the stone on CT imaging such as the attenuation, or Hounsfield measurement, may be helpful when determining stone fragility and stone composition. Staghorn calculi branch into multiple calyces and are often designated as ‘partial’ or ‘complete’ depending on the size of the stone and number of calyces occupied. There is no clear consensus on what defines a partial versus a complete staghorn calculus, such as volume criteria or a number of calyces occupied. However, a staghorn calculus is generally considered a branching renal stone that occupies multiple portions of the renal collecting system.
Operative management:
Complete removal of staghorn calculi should remain the goal in patients whose comorbidities do not preclude treatment. Treatment options for staghorn calculi include PCNL, shock wave lithotripsy (SWL), ureteroscopy, or a combination of two or more of these treatments. Less commonly, invasive open or laparoscopic/robotic-assisted stone surgery is indicated. Irrigation of the collecting system with agents to dissolve stones, such as Renacidin®, with or without surgery has also been evaluated but is not commonly used. Important considerations when determining the ideal treatment for staghorn calculi include stone-free rates, number of required procedures, and complication rates. PCNL remains the gold standard first-line treatment for the majority of staghorn calculi. With the advent of less invasive procedures, miniaturized equipment, and better fragmentation and extraction devices, surgical management of these complex stones continues to improve. Complex or Staghorn Renal Calculi, are removed by a fine hole placed into the kidney.
Robotic and laparoscopic
Robotic and laparoscopic approaches have been adapted from open surgical techniques for the removal of large renal stones. These approaches require renal hilum exposure, renal vessel clamping, nephrotomy, collecting system closure, and parenchymal closure. Laparoscopic ultrasound may be used for intraoperative assessment of remaining stone fragments since fluoroscopy is not feasible during robotic surgery. While these techniques have been shown to be feasible with relatively good stone-free rates, they remain second-line therapies when compared with less invasive endourological techniques secondary to cost and lack of outcomes demonstrating superiority.
BEST UROLOGY HOSPITAL IN HYDERABAD FOR UROLOGY TREATMENT AND UROLOGY DISEASES
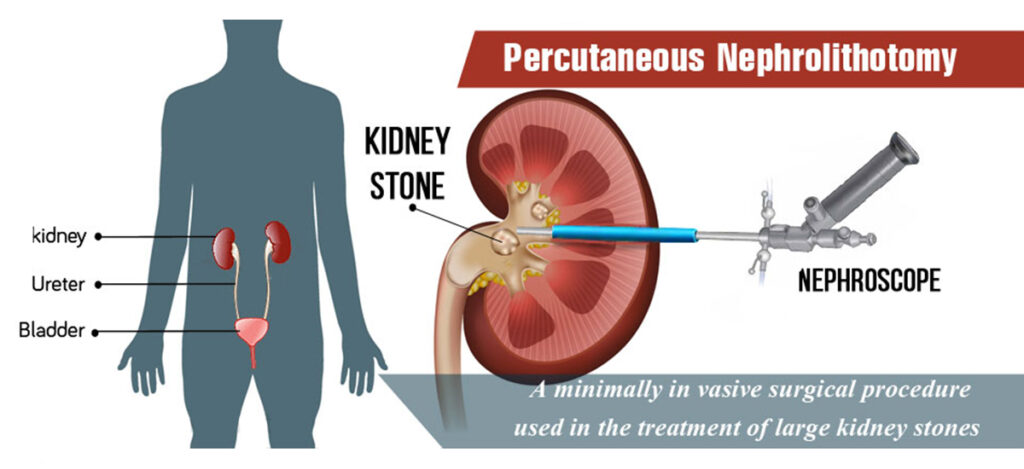
PCNL(Percutaneous Nephrolithotomy)
PCNL remains the gold standard treatment for staghorn calculi due to high stone-free rates and lowest complication rates. Optimal access to the kidney is imperative to successfully clear the collecting system of stone. Gaining access through the upper or lower pole calyces appears to be the best approach because it provides a straight track along the axis of the kidney and allows for access to the upper pole, lower pole, and the renal pelvis without excessive torquing of the rigid instruments.
Access should be gained below the level of the 11th rib and access should be obtained when the patient is kept under full expiration to minimize the risk of hydrothorax or injury to the lung. Multiple percutaneous access tracts may be utilized when treating large or complex stones. When used judiciously, multiple access tracts are safe and effective at achieving stone clearance with similar complication rates when compared with single-tract PCNL.
Nephrostomy tube drainage after a PCNL procedure is often recommended and serves multiple purposes. It can provide hemostatic tamponade of the tract, provide reliable drainage of the collecting system, and maintain access for future percutaneous procedures. Large bore nephrostomy drainage (>20Fr) may be reserved for patients who have significant bleeding or for patients with a high concern for infection. Small-bore (9–12Fr) nephrostomy drainage is more traditionally used. Tubeless PCNL is an option in uncomplicated cases and is associated with less postoperative pain and decreased hospital stay.
Why PCNL? – Conclusion.
PCNL (Percutaneous Nephrolithotomy) has remained the gold standard when treating these complex stones and the advent of smaller instruments and sheaths have broadened the arsenal of tools urologists have to completely clear these stones from the collecting system.
