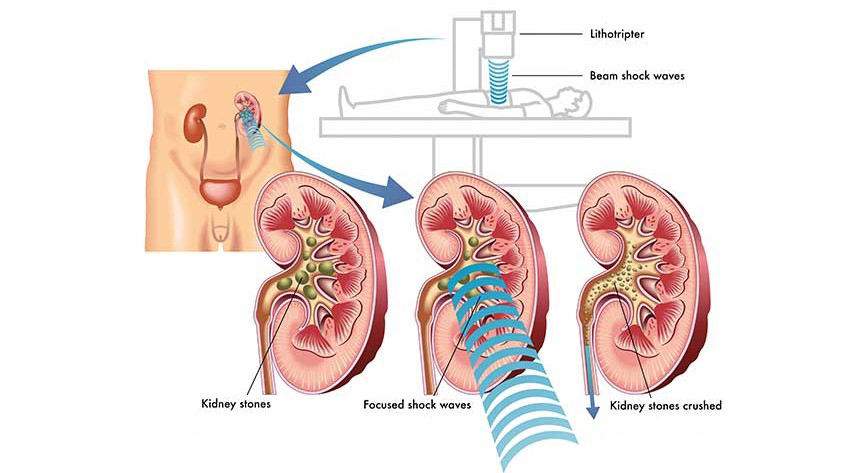
ESWL uses shock waves to break a kidney stone into small pieces that can more easily travel through the urinary tract and pass from the body.
History of Extracorporeal Shock Wave Lithotripsy
Thirty years after its introduction, extracorporeal shockwave lithotripsy(ESWL) is still first-line treatment for more than half of all urinary tract stones, but machines and treatment strategies have significantly developed over time.
is still first-line treatment for more than half of all urinary tract stones, but machines and treatment strategies have significantly developed over time.
In 1966, During Dornier’s research in aerospace technology, he discovered a previously unexplained phenomenon. Pitting of airplanes in the direction of the sound barrier- a unique event caused by the shock wave created in front of a droplet of vapor.
The Dornier Company explored the phenomenon initially, and later in partnership with the University of Munich.
Following extensive experimental testing on animals that provided the safety and reproducibility of a vivo shock wave, the first clinical application of ESWL performed on the 2nd February 1980 in Munich, Germany.
Dornier produced this human prototype, The HM1 (human-machine 1).
The HM3 became available in 1984 and since then several generations of lithotripters have been introduced. They differ in their means of shock wave generation and other minor areas such as table design.
All modifications have been in an effort to improve the success rates of the stone fragmentation, decrease patient morbidity and improve ease of use.
Imaging in ESWL
In order to treat the stone, it must first be visualized. This can be done using either fluoroscopy or ultrasound imaging. The fluoroscopy used is more multiplane in order to judge the depth of the target.
This can be used with either antegrade or retrograde contrast media for difficult-to-visualize calculi, although the use of contrast media is rare as it typically only shows a filling defect which indicates a large stone.
Large stones are rarely a problem to visualize (Lucas, Zheng, & Gravenstein, 2014). Ultrasound can be used, and it has been incorporated into some machines.
it uses no ionizing radiation and allows the treatment of radiolucent stones, which fluoroscopy does not.
it uses requires considerable skill and experience of the operator and, due to the interference and location of skeletal structures such as ribs, not all stones in the renal collecting system can be visualized.
Furthermore, it can be difficult to judge the degree of fragmentation during the ESWL treatment as a collection of crushed sand and gravel will appear remarkably similar to a solid stone on ultrasound whereas on fluoroscopy this can be better identified.
ESWL in children
For urolithiasis in children, ESWL shows excellent results and has therefore traditionally been the first-line treatment even for large stone burdens.
This is because the pediatric ureter is shorter and more elastic, and therefore has a higher stone-transporting capacity, such that even staghorn calculi can be cleared after a few sessions, and in most cases, stenting is unnecessary.
However, the current EAU guidelines, PCNL recommended for larger stones (>20 mm) and the same stratification criteria are applied as for adults.
